 WHAT IS A COLONOSCOPY?
WHAT IS A COLONOSCOPY?
Colonoscopy is a test that allows Mr Klaassen to examine your large bowel with a fine flexible telescope. This test will review your bowel from the rectum to the cecum and the end of your small intestine called the terminal ileum.
Why am I having the procedure? Your doctor may have referred you for a colonoscopy in order to investigate some symptoms you have been having, such as a change in bowel habit, rectal bleeding; or to review a problem they may have found before, like polyps or colitis. This will benefit you by providing a clear diagnosis.
There are other methods of examining the colon, such as a barium enema or a CT scan. Colonoscopy allows biopsies to be taken and procedures such as the removal of polyps to be performed.
WHAT PREPARATION WILL I NEED?
When you book your appointment, the reception staff will give you some preparation to take the day before your colonoscopy. The preparation may come in sachets or bottle form, and works as a powerful laxative to make your bowel completely clean. This allows Mr Klaassen to have a clear view of your bowel. We will give you instructions with the bowel preparation. You will not be allowed to eat any food for up to 24 hours before your procedure.
However you must drink lots of clear fluids, stopping 3 hours before the procedure. It is of great importance that this preparation works, or the test will not be possible. What should I bring on the day? Please bring all your medication and a dressing gown. What about my medications? If you are taking iron tablets, please stop them 7 days before your test.
If you are taking anti-inflammatory tablets (such as neurofen, brufen or voltarol) please stop taking them 5 days before your test.
Do not stop taking aspirin, clopidogrel or warfarin but please make sure that you have discussed this with your referring doctor before the test. There is a significant risk that a coronary stent will block if these medicines are stopped within one month of stent placement; and a slightly increased risk within the first six months. If the referring doctor thinks it is in your best interests to stop taking them, they should be stopped 10 days before the colonoscopy.
If you are a diabetic, please let Mr Klaassen know. He will give you more detailed information about your preparation.
Women taking the oral contraceptive pill should be aware that taking bowel preparation might prevent the absorption of the pill. Additional contraceptive precautions should be taken until the next period begins.
WHAT HAPPENS ON THE DAY OF THE TEST?
Please book in with the endoscopy reception staff when you arrive. Please do not have anything to drink for 3 hours before you arrive. They check your personal details, such as your name and address. We try to ensure that all patients are seen and have their tests within a short period of time of arriving.
Next, Mr Klaassen talks you through the consent form and the potential complications. It is important for you to think about these in advance so when you sign the form you are comfortable that it is a test you really want. Remember, you can change your mind about having the test at any time. Please tell Mr Klaassen if you have heart valve disease or if you are normally given antibiotics when you visit the dentist.
One of the endoscopy nurses then sees you, asks you some further questions, checks you have taken your preparation correctly and answers any questions you may have. Then the nurse asks you to get changed into a gown and shows you into the endoscopy room.
The doctor or nurse puts a small needle into the back of your hand. This is to give you sedation and painkillers. These drugs are used together to reduce your discomfort and make you a little sleepy. This is not a general anaesthetic.
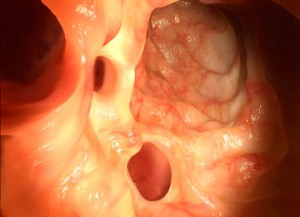
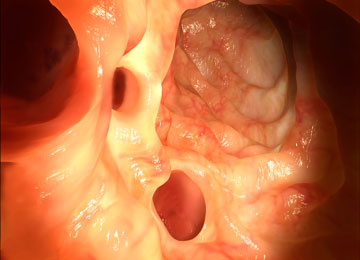
Once the medications have taken effect Mr Klaassen inserts a flexible tube (the endoscope) with a light on the end of it into your back passage. It is thinner than an index finger. Your bowel is inflated with air, and you may experience some bloating and discomfort. The tube is slowly moved along your colon whilst he gets a good look at the wall of the bowel. The tube travels right around the colon to the cecum. The test usually takes 20 – 30 minutes.
During the test Mr Klaassen may take biopsies (tissue samples), photographs or video of your bowel, even if it all looks normal. There may be periods of discomfort as the tube goes around bends in the bowel. Usually these will ease once the bend has been passed. If you are finding the procedure more uncomfortable than you would like, please let the nurse know and you can be given some more sedative or painkiller. In order to make the procedure easier you may be asked to change position (for example, to roll onto your back).
There will be a nurse with you throughout the procedure explaining what is happening, monitoring your vital signs, level of comfort and assisting the doctor. What happens if a polyp is found? One of the aims of colonoscopy is to detect polyps. Polyps are very small growths that can occur on the bowel wall. Some are perfectly innocent, but others can develop into bowel cancer if they are not removed. Consequently, polyps are removed, which most of the time is entirely safe. This is termed a polypectomy. In addition, sometimes thermal coagulation is used to destroy polyps or abnormal blood vessels.
WHAT ARE THE COMPLICATIONS OF COLONOSCOPY?
Complications are rare, but it is important that you know all the risks before you decide to go ahead with the test. Despite using sedation and pain killers some patients can experience abdominal discomfort or pain.
In approximately 1 in 10 patients the procedure is difficult and the doctor finds it impossible to look right around the bowel. If this happens Mr Klaassen may organise another test.
There is a very small risk of making a hole in the bowel wall (a perforation). This occurs in approximately 1 in 800 examinations. Perforations usually need to be repaired with an operation, and might require a temporary stoma (a surgical constructed opening, that permits the passage of waste).
If the doctor removes a polyp, then the risk of perforation, though still rare, increases slightly to about 1 in 600 occasions.
Bleeding from the rectum occurs in about 1 in 1500 cases, although if a polyp is removed it occurs in between 1 in 50 and 1 in 100 cases. It usually stops without any treatment but can occasionally need an operation to repair the area.
Using sedation can cause breathing complications in 1 in 200 procedures, which usually are not serious. To reduce this risk, we monitor your pulse and oxygen levels throughout the test.
If you have severe pain, black tarry stools or persistent bleeding, you should contact your nearest A&E for further advice and also inform us.
WHAT HAPPENS AFTER THE TEST?
You are moved into the recovery area where a nurse monitors you for 1-2 hours whilst you sleep off the sedation. You may then eat and drink normally. You may feel a little discomfort due to the air in your abdomen – this is normal.
If you are going home the same day you must arrange for someone to escort you home. Be aware that parking at the hospital is very limited. If no escort is available, please bring enough money to pay for a taxi.
We strongly advise that you do not drink alcohol, operate machinery, drive or make important decisions for 24 hours after your procedure as sedatives can impair your judgement.
You can resume normal activities, work etc the following day.
HOW WILL I GET THE RESULTS?
Mr Klaassen will be able to tell you the results after the procedure. If you had sedation, it is a good idea to have someone with you when this occurs because the sedation can make you forget what is discussed. If biopsies were taken or polyps removed, you will be told the final diagnosis at a followup consult. These results may one week to come through. Copies of your colonoscopy report will be sent to your GP.